The right upper lobe bronchus lies higher than the left, and the left pulmonary artery lies higher than and posterior to the right pulmonary artery.
Magnified views of the hilar anatomy (lower panels). Asterisks on the magnified frontal view mark the upper lobe bronchi. The left main bronchus is twice as long as the right main bronchus in this individual
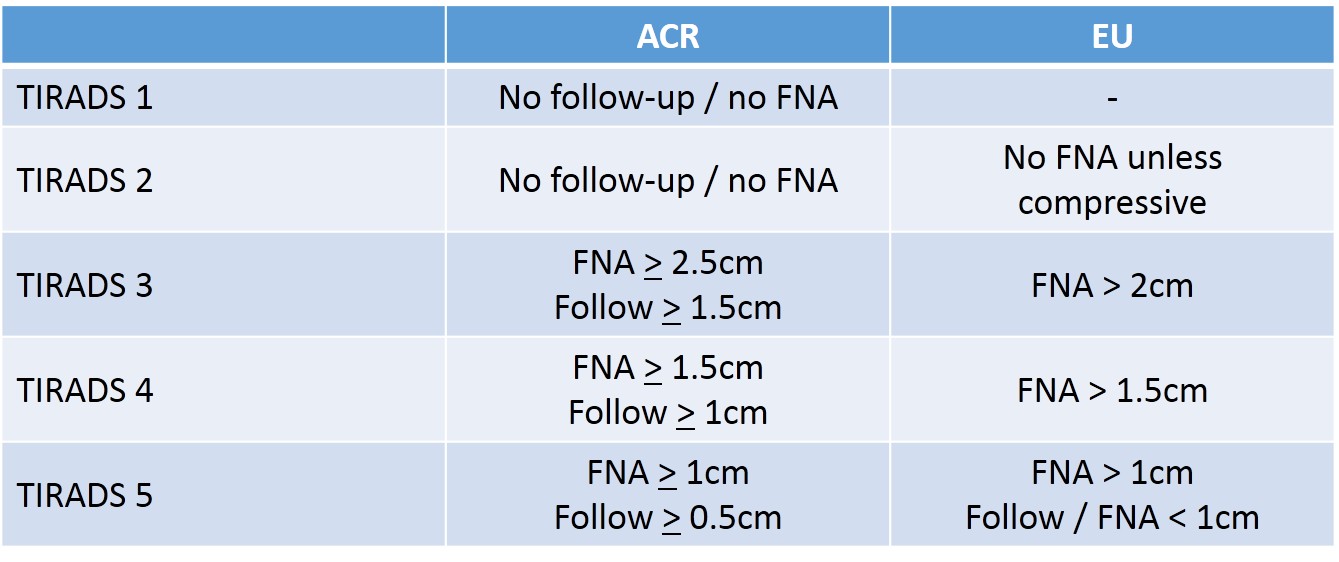
In this category, thyroid US should suffice to assert benignity without the need for FNA.
Purely Cystic Nodules.
In this category, thyroid US should suffice to assert benignity without the need for FNA.
Purely Cystic Nodules.
In this category, thyroid US should suffice to assert benignity without the need for FNA.
Purely Cystic Nodules.Absence of wall thickening or a solid component; disregard their size. This category includes cysts which are split into separate compartments by a few traversing septa. The presence of echogenic material inside the cyst is frequently encountered and can correspond either to a fibrin clot or a true solid component, which may be differentiated by the application of Doppler US. If doubt persists regarding the existence of a solid component, the nodule should be included in the low-risk category.
Spongiform Nodules. Composed of tiny cystic spaces involving the entire nodule; disregard their size; separated by numerous isoechoic septa. If the cystic spaces do not involve the entire nodule, the nodule should be considered as low risk.
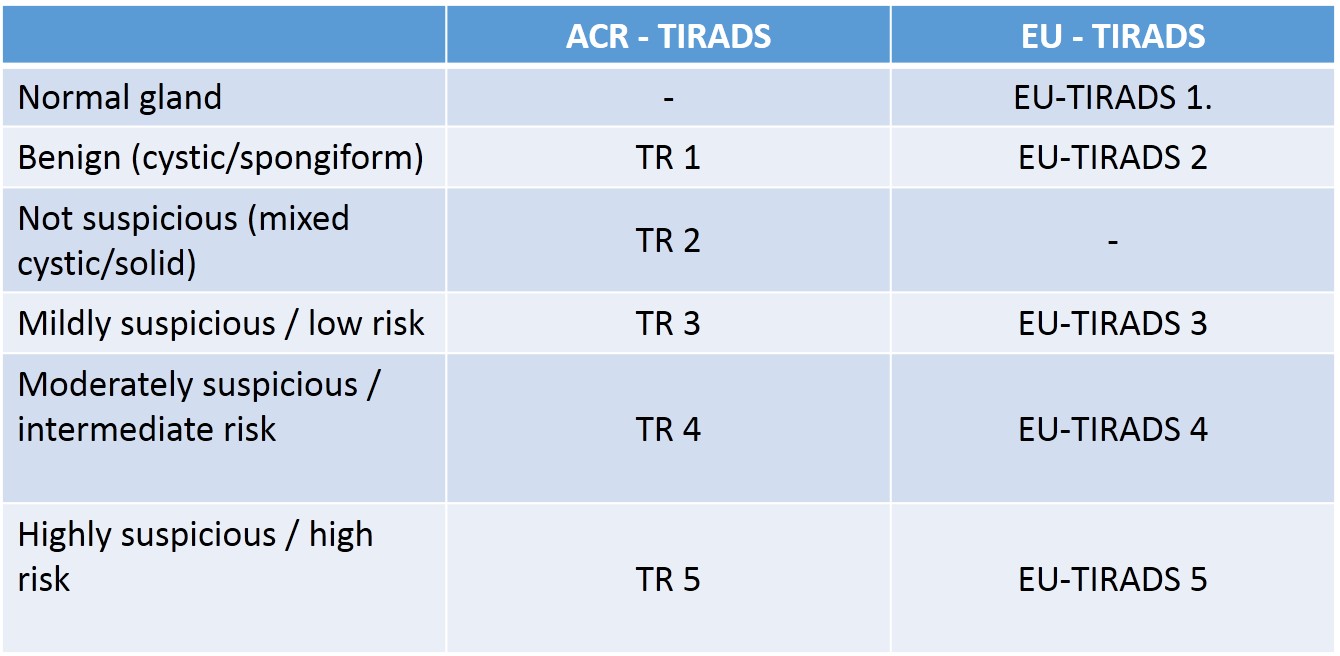
Low-Risk Category (EU-TIRADS 3)
Risk of malignancy: 2–4%
Definition
Pattern. Oval shape, smooth margins, isoechoic or hyperechoic, without any feature of high risk
.
EU-TIRADS 3: low-risk isoechoic nodule with an oval shape and smooth margins without any high-risk features.EU-TIRADS 3: low-risk hyperechoic nodule with an oval shape and smooth margins without any high-risk features.EU-TIRADS 3: grouped low-risk isoechoic nodules with an oval shape and smooth margins without any high-risk features.
Nodules with these characteristics have a low risk of malignancy, and FNA should usually be considered only for nodules >20 mm. The 20-mm threshold has been chosen based on the argument that distant metastases are rarely observed arising from follicular cancers <2 cm [27].
Grouped/coalescing isoechoic nodules (Fig. 6) should be included in this category, and FNA should be considered if 1 or more of the nodules is >20 mm. It should be pointed out, however, that an entirely solid isoechoic nodule corresponds in <4% of cases to a follicular cancer or a follicular variant of PTC [28–31]. In contrast, even minimal cystic changes are in favor of benignity
Intermediate-Risk Category (EU-TIRADS 4)
Risk of malignancy: 6–17%
Pattern. Oval shape, smooth margins, mildly hypoechoic, without any feature of high risk
EU-TIRADS 4: intermediate-risk, mildly hypoechoic nodule with an oval shape and smooth margins without any high-risk features.
The difference between the low-risk and the intermediate-risk category lies in the echogenicity of the solid part of the nodule. In case of heterogeneous echogenicity of the solid component, the presence of any hypoechoic tissue classifies the nodule as intermediate risk.
Other features may modulate the risk of malignancy in this category. The presence of a thin halo, a partially cystic composition, comet-tail artifacts, peripheral vascularity, and low stiffness lower the malignancy risk. In the Korean TIRADS, partially cystic nodules are considered to be low-risk lesions regardless of their echogenicity, and only entirely solid hypoechoic nodules are included in the intermediate-risk category. However, the Korean low-risk category has a 3–15% risk of malignancy, which is closer to the intermediate-risk category as defined by the present ETA guidelines. Thus, we consider all hypoechoic nodules as intermediate risk, including those with cystic areas, while acknowledging that the risk is lower in partially cystic than in entirely solid nodules. Features such as discontinuous peripheral/rim macrocalcifications, a thick halo, predominantly central vascularity, and high stiffness could raise the malignancy risk. Given the intermediate risk of EU-TIRADS 4 nodules, the task force chose to define the threshold for FNA in that group as 15 mm, which is in between the thresholds given for EU-TIRADS 5 and EU-TIRADS 3 nodules.
High-Risk Category (EU-TIRADS 5)
Risk of malignancy: 26–87%
Pattern. Nodules with at least 1 of the following high-risk features: non-oval shape, irregular margins, microcalcifications, and marked hypoechogenicity .
EU-TIRADS 5: high-risk nodule with a taller-than-wide shape, irregular margins, microcalcifications, and marked hypoechogenicity.EU-TIRADS 5: high-risk nodule with a non-oval shape, spiculated margins, microcalcifications, and marked hypoechogenicity. EU-TIRADS 5: two different examples of high-risk hypoechoic nodules with lobulated margins in the transverseEU-TIRADS 5: high-risk nodule with a taller-than-wide shape.
Background and Comments
These four US features were originally described in 2002; the average malignancy risk of such nodules was around 56% [6], but increasing with the number of suspicious features [15, 26]. This partly explains the wide range of malignancy risk in this category. All these characteristics show high rates of specificity (83–84%), but also low rates of sensitivity (26–59%) [6]. Marked hypoechogenicity has the lowest sensitivity of the four features, and is only specific if the nodule is solid and not the scar of a healed cyst [34]. The value of these features is also dependent on composition [16]. In partially cystic nodules, microcalcifications are the best predictor of malignancy, whereas other features seem less significant [16]. The number of spiculations, lobulations, or punctate echogenic foci has to be taken into account to gain specificity, which increases with the number of these anomalies.
All such nodules >10 mm should undergo FNA, unless a patient is inoperable or has a low life expectancy from other comorbidities. In case of a first benign cytological result, FNA should be repeated within 3 months to reduce the rate of false-negative samples.
In case of subcentimeter nodules with high-risk US features, active surveillance is recommended, provided that there are no abnormal lymph nodes and the patient is willing to accept regular US scanning. It is known that few or none of these patients will develop distant metastasis or die of their disease even if the nodule corresponds to a carcinoma [35]. In case of proven growth or detection of a suspicious lymph node during surveillance, FNA should be performed.
Recommendation
R5: Nodules having at least 1 suspicious US feature (i.e., a non-oval shape, irregular margins, microcalcifications, or marked hypoechogenicity) should be considered at high risk of malignancy, increasing with the number of suspicious features. FNA should be performed for nodules >10 mm.
* FNA should be performed in case suspicious lymph nodes are found.
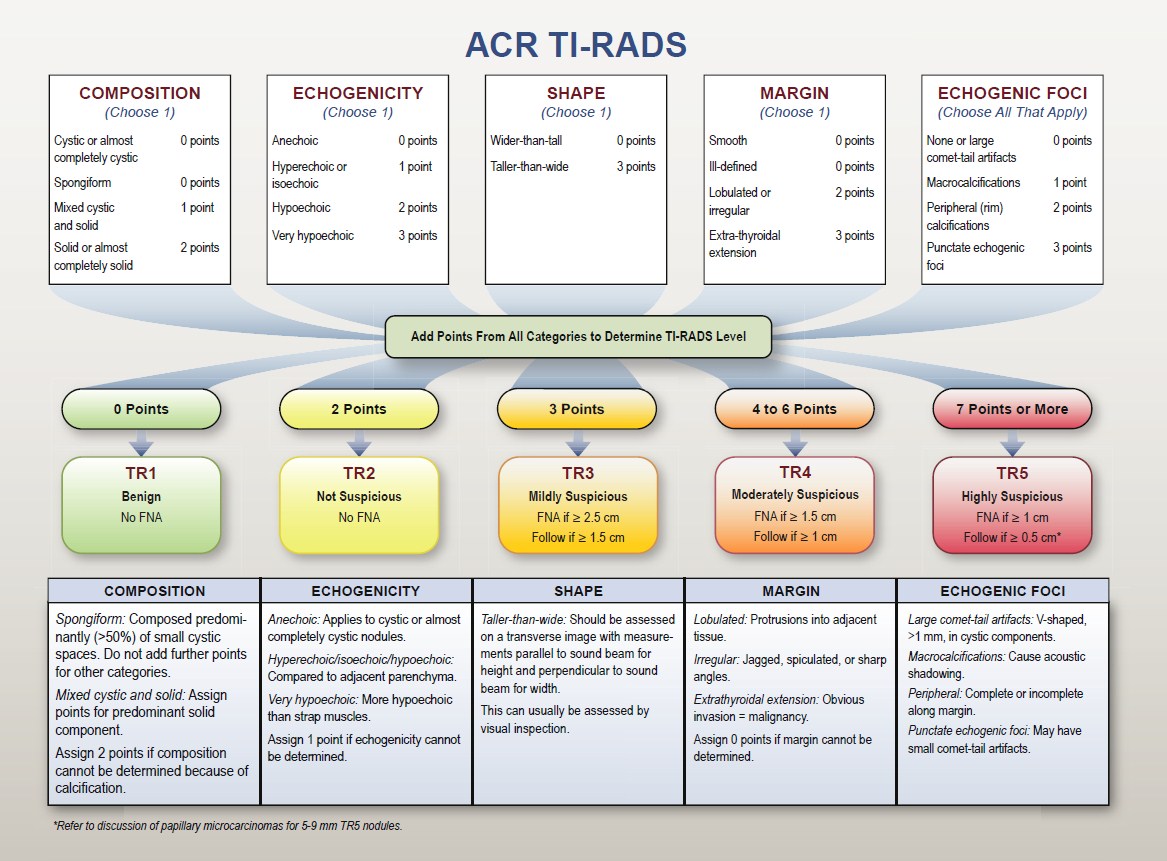
Macrocalcifications
Macrocalcifications can be defined as echogenic foci >1 mm in size with posterior shadowing. Three different patterns can be described:
Central intranodular macrocalcifications alone: not consistently associated with malignancy
Isolated macrocalcification, occupying an entirely calcified nodule: low risk
Rim (peripheral or curvilinear) or eggshell calcifications at the nodule margin: may increase the malignancy risk if disrupted
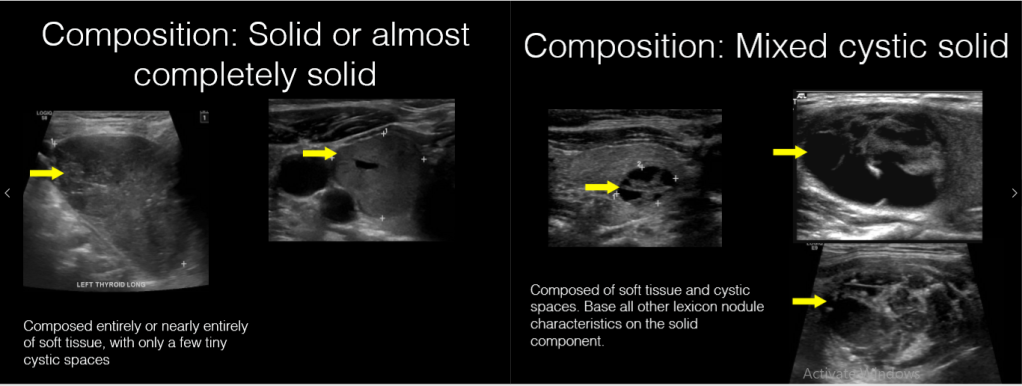
Composition: proportion of soft tissue or fluid in a nodule
Solid: composed almost entirely of soft tissue with <10% of liquid
Mixed predominantly solid: liquid component >10 but <50% of the nodule volume
Mixed predominantly cystic: liquid component >50 but <90% of the nodule volume
Cystic: composed entirely or nearly entirely of liquid
Spongiform appearance: tiny cystic spaces separated by thin septa
Comet tail: echogenic foci showing comet-like echogenic tails generated by reverberation artifacts within the cystic component
Egg shell calcification: echogenic line surrounding the nodule giving the appearance of a discrete calcified wall, along with marked posterior acoustic shadowing
Echogenicity: (in case the echogenicity of the surrounding thyroid tissue is decreased, such as in Hashimoto thyroiditis, the echogenicity of the solid component can be described relative to the normal submandibular salivary glands)
Mildly hypoechoic: refers to an appearance darker than the normal surrounding thyroid parenchyma, but less dark than the surrounding strap muscles
Isoechoic: similar brightness to the surrounding thyroid parenchyma
Markedly hypoechoic: refers to an appearance of the nodule darker than the surrounding strap muscles
Hyperechoic: brighter appearance than the surrounding thyroid parenchyma
Echotexture: characterizes the uniform or multiform appearance of the solid portion of a nodule
Heterogeneous: mixed isoechoic and hypoechoic echogenicity of the solid portion of a nodule
Homogeneous: uniform appearance of the solid portion of a nodule
Halo/rim: sonolucent black outline that surrounds a nodule; can be described as thin or thick
Macrocalcification: >1-mm coarse and large calcification with posterior acoustic shadowing
Microcalcification: <1-mm, most often round calcification
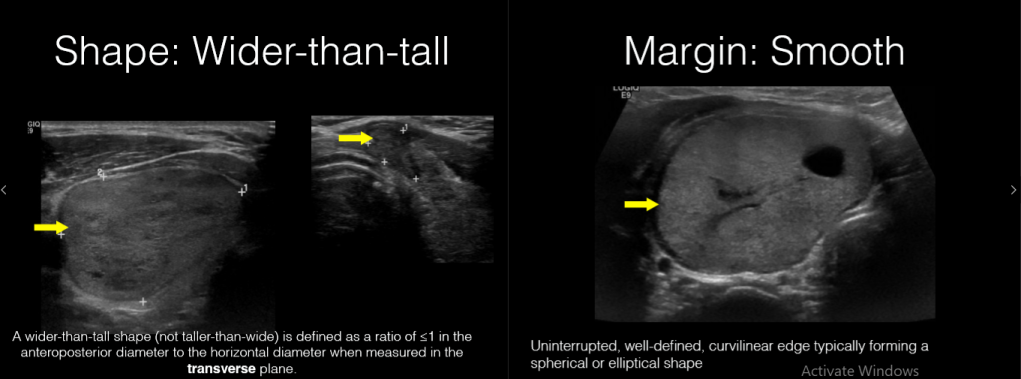
Margin: describes the outline of the thyroid nodule
Smooth margin: clear demarcation to the surrounding thyroid parenchyma
Ill-defined margin: lack of a clear demarcation to the surrounding thyroid parenchyma; ill-defined margins are distinct from irregular ones and do not alter the nodule’s risk category
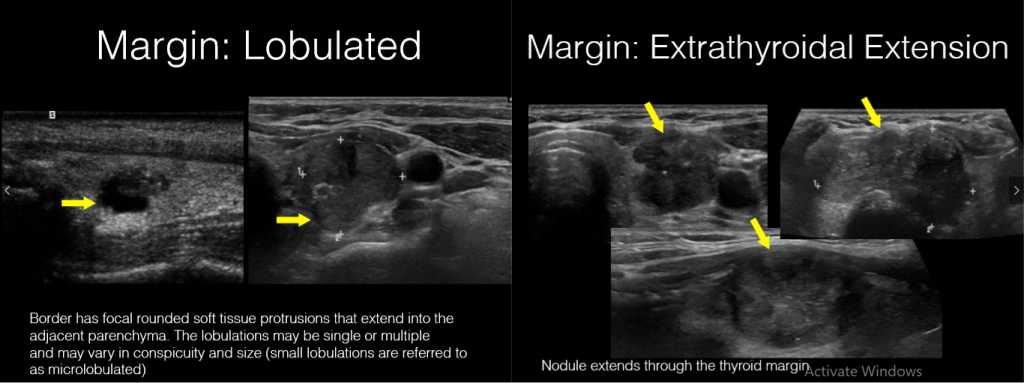
Irregular margin:
Spiculated: presence of 1 or more sharp angles or spiculations on the margin
Microlobulated: presence of 1 or more smooth, focal, round protrusions on the margin
Nodule:nodulus (Latin) – small knot; lump
Shape:
Oval shape: the anteroposterior diameter of a nodule is less than its transverse diameter on the transverse and longitudinal planes
Round: the anteroposterior diameter of a nodule is equal to its transverse diameter on the transverse and longitudinal planes
Taller than wide: the ratio of the anteroposterior-to-transverse diameter of a nodule is >1
Taller than long: the ratio of the anteroposterior-to-longitudinal diameter is >1
Vascularity:
Type I: absence of intranodular or perinodular flow
Type II: presence of perinodular and/or slight intranodular flow
Type III: presence of marked intranodular and slight perinodular flow
The Antenatal Presentation (left column) is divided into normal, A1 and A2-3, and measurements between 16–27 weeks’ and ≥ 28 weeks’ gestation. A normal urinary tract is one with no urinary tract abnormalities and anterior posterior renal pelvic diameter (APRPD) measuring less than 4 mm between 16–27 weeks’ gestation and less than 7 mm ≥28 weeks’ gestation
A1 describes a normal urinary tract with 4 to <7 mm pelvic dilation at 16–27 weeks’ gestation or 7 to <10 mm ≥28 weeks’ gestation with or without central calyceal dilation. UTD A2-3 is for fetuses if there is APRPD ≥7 mm between 16–27 weeks’ gestation or ≥10 mm ≥28 weeks’ gestation, peripheral calyceal dilation, ureteral dilation, renal parenchymal or bladder abnormalities.
The Postnatal Presentation (right column) is divided into normal, P1, P2 and P3. Measurements are more reliable if taken 48 h after birth or later.A normal urinary tract is one with no urinary tract abnormalities and APRPD <10 mm. P1 describes a normal urinary tract with APRPD 10 to <15 mm and/or central calyceal dilation. P2 describes APRPD ≥15 mm or peripheral calyceal dilation.P3 describes additional ureteral dilation, abnormal renal echogenicity or cysts or bladder abnormalities regardless of APRPD measurement.